
Physiology and Risk at High Altitude
In a span of 43 days, Capitol Peak became the deadliest mountain in Colorado, claiming the lives of 5 people. The number of fatalities in 2017 was in fact unusual. 11 deaths statewide on 14,000 ft. peaks (commonly referred to as 14ers), has provoked communities all over Colorado to question: why is this happening? Popularity in summiting 14ers has skyrocketed in the last 3 decades. In 2007, it was estimated that 200,000 people attempted at least one 14er, a 300 percent increase since 1987. This number continues to grow with the boom in tourism, access to hiking information, and behavioral motivators such as sharing content on social media and athletic pursuit. The majority of 14er deaths involve a fatal fall on rock, snow, or ice. The cause of these falls, however, is vitally important and needs to be addressed.
Route on Capitol Peak
Many 14ers are easy to access and non-technical to climb, while others require an advanced skill set for successful attempts at the summit. With a majority of fatal accidents occurring on technically difficult routes, such as Capitol Peak, a compelling argument persists that too many unexperienced climbers are exceeding their abilities. This may contribute to a few cases of accident; however, this argument is far too simplistic. According to the American Alpine Journal, only 5.4% of accidents by immediate cause between 1951-2015 are attributed to climbers exceeding their abilities. Furthermore, accidents appear to occur across all levels of experience.
According to the Institute for Altitude Medicine in Telluride, CO, between 15 and 40% of visitors sleeping at 8000 ft. or higher experience Acute Mountain Sickness (AMS). Additionally, it has been reported that 60% of visitors sleeping at 9800 ft. experienced a high-altitude headache. Despite high prevalence of reported signs of altitude sickness, only 3.2% of US Mountaineering injuries are attributed to high altitude illnesses including AMS, High Altitude Cerebral Edema (HACE), and High Altitude Pulmonary Edema (HAPE). The aim of this article is to discuss the impact of altitude on cognitive, motor, and cardiorespiratory functioning that occurs before a diagnosis of altitude sickness. A further understanding of impairment occurring independent of altitude sickness will shape how we view climbing and decision making at high altitude.
What adaptations occur upon ascent to altitude?
Upon ascent to high altitude, there is a deficit in oxygen availability due to decreased atmospheric partial pressure of inspired oxygen (PO2). At 4,000 m, (~13,100 ft.), the PO2 is only about 60% of the value at sea level. This decrease in oxygen availability, known as hypoxia, triggers numerous concomitant responses of the cardiovascular, respiratory, muscular, endocrine and neural systems in an effort to maintain homeostasis. The oxygen transport cascade consists of a series of actions that involve transport of oxygen from environmental air to the mitochondria to maintain aerobic metabolism. Abnormally low levels of oxygen in the blood, known as hypoxemia, is first detected in the carotid arteries, our 'fight-or-flight' response is initiated by the sympathetic nervous system. To match oxygen delivery with metabolic demand, an increase in heart rate and ventilation is mediated by the sympathetic nervous system during rest and exercise.
Heart rate increases in an effort to maintain cardiac output and oxygen consumption. Upon ascent to altitude, there is a rapid loss of blood plasma volume, which occurs as a compensatory mechanism to increase hematocrit, the ratio of red blood cells to total blood volume. This adaptation increases blood viscosity and lowers stroke volume, which causes the heart to beat faster to maintain adequate cardiac output.
The immediate increase in ventilation at altitude acts to compensate for the low PO2 gradient in the alveoli by creating a stronger "driving-force" of oxygen entering pulmonary circulation. This response, termed the Hypoxic Ventilatory Response, is crucial for acclimatization, however, the energy demands of sustaining hyperventilation have compensatory implications on performance and well-being.
Decline in Exercise Performance at Altitude
Volume of oxygen consumption (VO2) is a measure of the amount of oxygen that is utilized to convert energy from calories we consume into energy molecules called adenosine triphosphate (ATP). When we begin exercising or increase exercise intensity, there is a greater metabolic need for ATP. Maximal oxygen uptake (VO2max) refers to the highest rate at which oxygen (O2) can be taken up and consumed by the body during intense exercise (Bassett & Howley, 2000). VO2max is the ultimate measure of cardiorespiratory and metabolic functioning and also indicates success in endurance performance. VO2max declines linearly approximately 10% for every 1000 m above 1500 m (Fulco, Rock, & Cymerman, 1998). With increasing altitudes, there is a decrease in the partial pressure of O2 due to less overlying atmospheric mass. As an individual ascends higher, the pressure gradient of oxygen entering the alveoli decreases, and therefore, the driving force of oxygen consumption is impaired.
While exercising at altitude, the respiratory system requires supplemental blood flow to sustain the energy demands of hyperventilation. For instance, at sea level about 5% of your cardiac output is used for breathing during rest. If you were going to travel up to 16,000 ft., 26% of your cardiac output is used during rest. Redistributing cardiac output from the working muscles to support the energy demands of respiratory muscle is known as the “blood steal effect” (Harms et al., 1997). Due to less available blood flow for working muscles, a shift from aerobic (with O2) to anaerobic (without O2) respiration occurs to match energy production with metabolic demands of exercise. Glucose and stored glycogen become the preferred fuel source during exercise due to increased sympathetic drive and the greater yield of ATP per liter of O2 consumed. However, glucose and glycogen represent a relatively smaller fuel source and consequently produce a greater yield of waste products such as hydrogen ions and carbon dioxide (CO2). Greater reliance on anaerobic pathways for energy metabolism is associated with an earlier onset of peripheral fatigue and excessive hyperventilation during exercise. For instance, in a study investigating exercise performance in unacclimatized males at altitude, researchers observed excess hyperventilation and a greater reliance on anaerobic energy metabolism during a VO2max test. This shift in energy metabolism contributed to an earlier onset of metabolite accumulation and exhaustion during the test (Gudjonsdottir et al., 2001).
Excessive hyperventilation at altitude significantly reduces CO2 in the blood. CO2 is a potent vasodilator of cerebral vessels causing global cerebral blood flow to increase by 2-4% per mmHg rise in partial pressure of arterial CO2 (Fortune et al., 1992; Sato et al., 2012). Low CO2 in the blood, known as hypocapnia, causes alkalinity and subsequently leads to arterial vasoconstriction in the brain. It has been demonstrated that high-intensity exercise at altitude leads to hyperventilation-induced hypocapnia causing cerebral vasoconstriction (Subudhi, Dimmen, & Roach, 2007). Due to limited cerebral blood flow, a hierarchy of oxygen delivery develops via vascular resistances.
Delivery of oxygen is favored to brain centers associated with vital functioning such as the brainstem and hypothalamus. The brainstem is essential for survival as it regulates cardiac output, respiratory function, and consciousness. The hypothalamus is the link between the endocrine and nervous system and maintains homeostasis by regulating heart rate, blood pressure, body temperature, and fluid and electrolyte balance. Brain centers such as the prefrontal cortex and hippocampus are not involved in vital functioning and experience a significant decline in blood flow and oxygen delivery. This impairment in oxygen and nutrient supply subsequently weakens functioning and may influence decision making, situational awareness, and balance while climbing 14ers [see figure 2 for summary of physiological interactions].

Figure 2: Physiologic mechanisms of impaired decision making
Adapted from Fan & Kayser (2016)
Are we more likely to fall into heuristic traps at altitude?
Climbing in high-risk terrain presents individuals with complex and difficult problems requiring rational thinking and decision making. The process of making and executing decisions, both good and bad, is supported by human information processing [see figure 3]. In high altitude mountaineering, rational decision making is critical as a single mistake can easily cost you your life.
The rational part of the brain, the prefrontal cortex, responds to situations with the perspective of understanding long term consequences from immediate actions. It regulates impulse control, emotional input, and gratification postponement. The prefrontal cortex also integrates past experiences with current problems while making decisions. It's role in complex cognitive functioning is essential while navigating high risk terrain such as technical 14er routes.
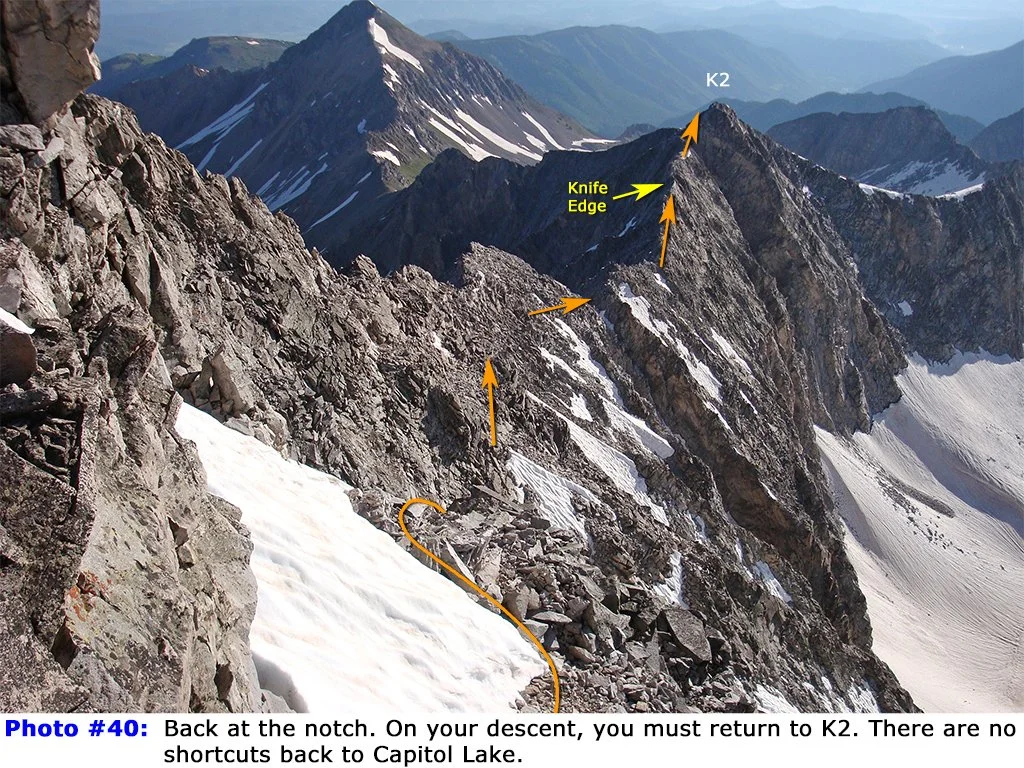
Subudhi et al. (2009) investigated oxygenation of the prefrontal, premotor, and motor regions during rest and exhaustive exercise at a simulated altitude of 4800 m. In hypoxia, prefrontal oxygenation was reduced 11% at rest and decreased another 26% at exhaustion. Researchers concluded that reductions in prefrontal oxygenation may limit exercise performance by impairing executive functions that influence the decision to stop exercising. While navigating mountain terrain, increased fatigue and impaired prefrontal cortex functioning may contribute to climbers making poor route-finding decisions. For instance, a majority of fatalities on Capitol Peak were attributed to climbers descending off-route on what was perceived to be a "short-cut." This route [pictured below] instead led off a 600-ft. cliff that could not be navigated without special mountaineering equipment. In this scenario, climbers may have been influenced by the emotional part of their brain, the amygdala, instead of making rational choices with their prefrontal cortex.
Emotional decision making rather than rational decision making often contributes to a set of heuristics known as the human factor. Human factors such as confirmation bias and cognitive inertia intensify when behavioral motivators inhibit our ability to analyze the relative danger of a situation in foresight. An archetype of mountaineering known as "summit fever," has repeatedly led climbers to neglect obvious signs to turn around. Continuing to summit despite obvious signs of an incoming storm or a missed turn-around time reveals that an individual is not thinking rationally. In summary, there is evidence to support exercise at altitude impairs a climber's ability to regulate emotional impulses and plan long term strategies to safely ascend and descent a 14er.
How is Situational Awareness Impacted at Altitude?
Situational awareness is the process of detecting and integrating environmental cues into one's perception of a dynamic situation. In essence, situational awareness is the degree of accuracy of our perception vs. reality. A mountaineer may focus their awareness on factors like: What is happening with the weather? What is the condition of the party? What is the condition of the route? Awareness of these factors is involved when making a specific situational assessment such as a go/no-go decision of an objective. Maintaining ongoing situational awareness during a climbing objective is highly intensive in its demands on memory.
Working memory is the component of short term memory that temporarily stores information within a small organ in the brain called the Hippocampus. At an altitude of 3800 m, spatial and working memory begin to decline with increasing altitude (Wilson, Newman, & Imray, 2009). Impaired prefrontal cortex functioning directly contributes to the decline of working memory. The role of the prefrontal cortex in memory is to code select information with importance so that it remains available for analysis (Lara & Wallis, 2015). For example, remembering details of potential incoming weather serves purpose for one's own safety. Having this information stored as working memory, one's attention should be directed to observe additional cues such as - which way is the wind blowing? What is happening with the temperature? Reduced attention to these details may be due to the inability to suppress other behavior influencing motives such as hunger, fatigue, or desire to summit a peak. Furthermore, when climbing in a group, observing and recognizing signs of altitude sickness in your climbing partners is critical. Failure to recall early indications such as labored breathing or impaired balance may danger the group later in the day when it is too late.
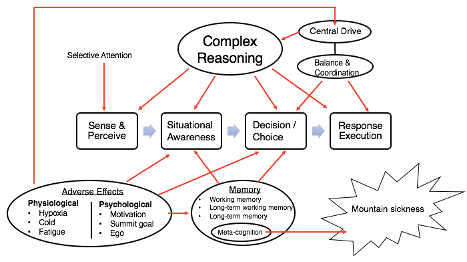
Figure 3: Information Processing Model of High Altitude Mountaineering Adapted from Wickens et al. (2015)
In a study investigating causal factors of deaths on Mount Everest between 1921-2006, a majority of deaths occurred during descent (Firth et al., 2008). While ascending a mountain, climbers develop a spatial map of their environment which includes details of the route such as major landmarks, loose rocks, and areas of exposure. Developing this spatial map of the environment is resource intensive, however, in high risk terrain - more detail the better. Retrieval of this information while descending is critical when the safest route is not clear, such as descent of a scree field after fogs rolls in. Furthermore, a climber's impression of how much control they have in a situation may be distorted, especially in familiar terrain. When making situational decisions, it is important to understand the dynamic nature of alpine terrain.
Are we more likely to fall?
Navigating high risk mountainous terrain that features loose rock, ice, and snow while carrying extra weight of gear has its own inherent risks. Compounding this with significant alterations in balance and ataxic gait indeed makes the climber vulnerable to trips or falls. Ataxia is the loss of coordination of voluntary body movements. It has been suggested that hypoxia contributes both directly and indirectly to the mechanisms underlying ataxia (Bird et al., 2011). The energy demands of neuronal conduction and requires large amounts of oxygen to function proper. Directly, hypoxia slows neuronal conduction and inhibits central drive, which affects muscle recruitment and movements involving coordination. Indirectly, the effect of hyperventilation-induced hypocapnic vasoconstriction reduces oxygen supply to brain areas involved in balance such as the basal ganglia and the cerebellum.
Ataxia is an early clinical feature of HACE. A clearly ataxic person cannot descend alone and therefore puts rescuers in danger. Attempts to correlate early signs of balance impairment with AMS have found that balance impairment occurs independent of AMS diagnosis, however, balance worsens with increasing altitude and diagnosis (Bird et al., 2011; Wilson et al., 2009). This implies a climber who is perceived to be non-affected by altitude may still experience balance impairment in high risk terrain.
How can we prevent accidents at altitude?
It has been well documented that pre-exposure to altitude, rate of ascent, and history of previous AMS are major independent determinants of the susceptibility of AMS. Altitude exposure for 5 days or more above 3000 m in the 2 preceding months of an ascent and following slow ascent rates (640 m gain of altitude or less per day above 2500 m) both reduce the risk of AMS by about 50% (Schneider, Bernasch, Weymann, Holle, & Bartsch, 2002). These recommendations, however, are often overlooked due to time constraints and other logistical reasons. When symptoms of mountain sickness are observed during a climbing objective [see table 1 for symptoms], a variety of pharmacological treatments are available such as Diamox and Dexamethasone. These drugs are effective at preventing and reducing the symptoms of mountain
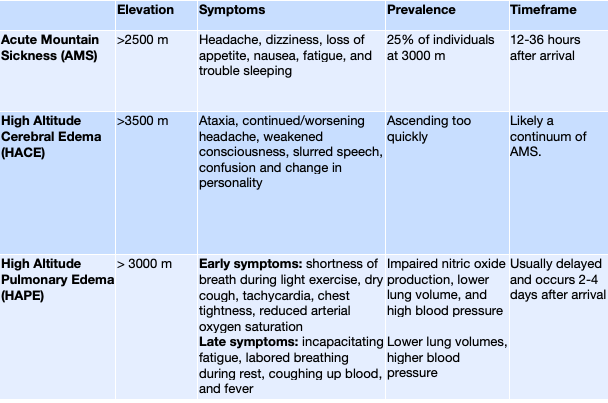
Table 1: Symptoms of Mountain Sicknesses
sickness but should only be used in high risk situations as they are associated with the risk of adverse side effects. If possible, the single best treatment is immediate descent to lower altitudes.
Developing effective, well-tolerated strategies that help attenuate the adverse effects of altitude and reduce the number of accidents remains to be an ongoing focus of research.
Understanding why native altitude populations tolerate altitude may help us advance this research focus. Evolutionary adaptations over the last ~25,000 years have assisted native Tibetan populations in thriving in their harsh environment of high altitude. Interestingly, functional adaptations in native Tibetans are distinct from native Andean populations who arrived in South America and have lived on the highlands of Bolivia and Peru for the last ~11,000 years (Beall, 2007; Jansen & Basnyat, 2011).
Native Tibetans are known for changes in their respiratory physiology such as higher resting ventilation and a stronger Hypoxic Ventilatory Response compared to native Andeans. This response contributes to greater oxygen uptake and higher levels of oxygen saturation at altitude. Native Andean populations are recognized for having higher hemoglobin concentrations and therefore a greater oxygen carrying capacity. However, exaggerated hemoglobin production, known as polycythemia, may lead to a condition called Chronic Mountain Sickness (CMS). CMS is characterized by extreme blood viscosity (hematocrit > 60%) and symptoms including fatigue, breathlessness, and cognitive impairment (Villafuerte & Corante, 2016). Ultimately, CMS leads to increased pulmonary artery pressure and a considerable risk of heart failure. It has been suggested that this condition is relatively rare in native Tibetans because they have significantly greater endogenous production of Nitric Oxide (NO) (Beall, Laskowski, & Erzurum, 2012; Erzurum et al., 2007).
NO is a potent vasodilator synthesized in the endothelium of blood vessels. NO synthesis is downregulated in low-altitude natives upon acute exposure to high altitude. This response induces pulmonary vasoconstriction and has been suggested as major contributor of HAPE (Bailey et al., 2010). Elevated NO synthesis in Tibetans leads to remarkable differences in pulmonary and cerebral blood flow. For instance, Jansen & Basnyat (2011) demonstrated that a Tibetans have 24% higher cerebral blood flow compared to Andean populations living at the same altitude. Furthermore, Norcliffe et al. (2005) suggested that impaired release of NO contributed to a larger cerebral vasoconstrictive response to hypocapnia in Andeans at high altitude. Considering the benefit of NO in native Tibetans, a functional approach to increase the bioavailability of NO in low altitude natives should be considered in high altitude mountaineering.
Scherrer et al. (1996) demonstrated that inhaling NO for 15 minutes decreases systolic pulmonary artery pressure and improve arterial oxygenation in individuals prone to HAPE. However, this favorable response was apparent in HAPE prone individuals but not individuals resistant to HAPE. Unfortunately, breathing in NO impairs the partial pressure of inspired oxygen and may worsens oxygen saturation. How can we effectively increase NO availability in our blood?
High concentrations of dietary nitrate exist in beets, lettuce, collard greens, and many other foods. With the ingestion of these foods, you can increase the bioavailability of NO. Shannon et al. (2017) investigated the effect of dietary nitrates on cognitive function and exercise performance at high altitude. Participants consumed 140ml of concentrated BRJ before exercising in simulated high (3,000 m) and very high altitudes (4,300 m). Nitrate supplementation improved oxygen saturation, exercise efficiency (less oxygen required for a given activity), and improved time trial performance at both altitudes. Although no benefit in cognitive function was reported, other studies have reported enhanced cerebral oxygen delivery and improved executive functioning using dietary nitrates at low altitude (Gilchrist et al., 2014; Thompson et al., 2015).
Another method of increasing NO availability is a non-invasive clinical intervention known as ischemic pre-conditioning (IPC). It has been demonstrated that IPC usage before hypoxic exposure improves oxygen saturation, decreases hypoxic pulmonary vasoconstriction and attenuates the onset of AMS (Berger et al., 2015; Foster et al., 2014). IPC involves 5 min periods of occlusion and reperfusion of an arm or leg with a blood pressure cuff at 220mmHg. The sheer stress on the blood vessels triggers a hormetic response involving an immediate release of NO from the endothelium into the blood and an upregulation in NO production. Foster et al. (2014) administered IPC for 5 days prior to an ascent to altitude and observed significantly higher oxygen saturation, decreased pulmonary arterial pressure and faster finish time of a 12.8 km run at 4342 m. Interestingly, this improvement in oxygen saturation was sufficient enough to bring a person out of an oxygen saturation associated with sensory and mental decrement (75.3% vs. 80.3%).
The brain requires ~20% of the body's total energy to maintain proper functioning. In hypoxic environments, the oxidation of glucose into ATP for energy becomes impaired. This disruption undoubtedly contributes to impaired cognitive functioning while hiking a 14er. Creatine is recognized as a reserve energy substrate that can be used to replenish ATP without the need for oxygen. After ingesting 20 g of a creatine monohydrate supplement for 7 days prior to exposure to altitude, the concentration of creatine stored in the brain increased significantly (Turner, Byblow, & Gant, 2015). Cognitive functioning, particularly attentional capacity, was improved by 21% and subjects demonstrated greater analytical rational during stressful mental tasks. In a study investigating the effect of creatine supplementation on sleep deprivation, individuals ingesting creatine had greater movement generation, choice reaction time, balance, and mood (McMorris et al., 2006). Interestingly, creatine had a positive impact on tasks that place heavy stress on the prefrontal cortex.
Beet root juice, IPC, and creatine supplementation are preventative strategies that may improve performance, attentional capacity, and decrease symptoms of mountain sickness. Although these strategies may have efficacy, no strategy can replace patience, sound judgement and the years of experience it takes to respect the power of the mountains.
References
Bailey, D. M., Dehnert, C., Luks, A. M., Menold, E., Castell, C., Schendler, G., … Berger, M. M. (2010). High-altitude pulmonary hypertension is associated with a free radical-mediated reduction in pulmonary nitric oxide bioavailability: Redox regulation of hypoxic pulmonary vasoconstriction. The Journal of Physiology, 588(23), 4837–4847. https://doi.org/10.1113/jphysiol.2010.194704
Bassett, D. R., & Howley, E. T. (2000). Limiting factors for maximum oxygen uptake and determinants of endurance performance. Medicine and Science in Sports and Exercise, 32(1), 70–84.
Beall, C. M. (2007). Two routes to functional adaptation: Tibetan and Andean high-altitude natives. Proceedings of the National Academy of Sciences of the United States of America, 104(Suppl 1), 8655. https://doi.org/10.1073/pnas.0701985104
Beall, C. M., Laskowski, D., & Erzurum, S. C. (2012). Nitric oxide in adaptation to altitude. Free Radical Biology and Medicine, 52(7), 1123–1134. https://doi.org/10.1016/j.freeradbiomed.2011.12.028
Bird, B. A., Wright, A. D., Wilson, M. H., Johnson, B. G., Imray, C. H., & Society, B. M. R. E. (2011). High altitude ataxia—its assessment and relevance. Wilderness & Environmental Medicine, 22(2), 172–176.
Erzurum, S. C., Ghosh, S., Janocha, A. J., Xu, W., Bauer, S., Bryan, N. S., … Beall, C. M. (2007). Higher blood flow and circulating NO products offset high-altitude hypoxia among Tibetans. Proceedings of the National Academy of Sciences, 104(45), 17593–17598. https://doi.org/10.1073/pnas.0707462104
Firth, P. G., Zheng, H., Windsor, J. S., Sutherland, A. I., Imray, C. H., Moore, G. W. K., … Salisbury, R. A. (2008). Mortality on Mount Everest, 1921-2006: descriptive study. BMJ, 337(dec11 1), a2654–a2654. https://doi.org/10.1136/bmj.a2654
Fortune, J. B., Bock, D., Kupinski, A. M., Stratton, H. H., Shah, D. M., & Feustel, P. J. (1992). Human Cerebrovascular Response to Oxygen and Carbon Dioxide as Determined by Internal Carotid Artery Duplex Scanning: The Journal of Trauma: Injury, Infection, and Critical Care, 32(5), 618–628. https://doi.org/10.1097/00005373-199205000-00014
Foster, G. P., Giri, P. C., Rogers, D. M., Larson, S. R., & Anholm, J. D. (2014). Ischemic Preconditioning Improves Oxygen Saturation and Attenuates Hypoxic Pulmonary Vasoconstriction at High Altitude. High Altitude Medicine & Biology, 15(2), 155–161. https://doi.org/10.1089/ham.2013.1137
Fulco, C. S., Rock, P. B., & Cymerman, A. (1998). Maximal and submaximal exercise performance at altitude. Aviation, Space, and Environmental Medicine, 69(8), 793–801.
Gilchrist, M., Winyard, P. G., Fulford, J., Anning, C., Shore, A. C., & Benjamin, N. (2014). Dietary nitrate supplementation improves reaction time in type 2 diabetes: Development and application of a novel nitrate-depleted beetroot juice placebo. Nitric Oxide, 40, 67–74. https://doi.org/10.1016/j.niox.2014.05.003
Gudjonsdottir, M., Appendini, L., Baderna, P., Purro, A., Patessio, A., Vilianis, G., … Donner, C. F. (2001). Diaphragm fatigue during exercise at high altitude: the role of hypoxia and workload. European Respiratory Journal, 17(4), 674.
Harms, C. A., Babcock, M. A., McClaran, S. R., Pegelow, D. F., Nickele, G. A., Nelson, W. B., & Dempsey, J. A. (1997). Respiratory muscle work compromises leg blood flow during maximal exercise. Journal of Applied Physiology (Bethesda, Md.: 1985), 82(5), 1573–1583.
Jansen, G. F., & Basnyat, B. (2011). Brain blood flow in Andean and Himalayan high-altitude populations: evidence of different traits for the same environmental constraint. Journal of Cerebral Blood Flow & Metabolism, 31(2), 706–714.
Lara, A. H., & Wallis, J. D. (2015). The Role of Prefrontal Cortex in Working Memory: A Mini Review. Frontiers in Systems Neuroscience, 9. https://doi.org/10.3389/fnsys.2015.00173
McMorris, T., Harris, R. C., Swain, J., Corbett, J., Collard, K., Dyson, R. J., … Draper, N. (2006). Effect of creatine supplementation and sleep deprivation, with mild exercise, on cognitive and psychomotor performance, mood state, and plasma concentrations of catecholamines and cortisol. Psychopharmacology, 185(1), 93–103. https://doi.org/10.1007/s00213-005-0269-z
Norcliffe, L. J., Rivera-Ch, M., Claydon, V. E., Moore, J. P., Leon-Velarde, F., Appenzeller, O., & Hainsworth, R. (2005). Cerebrovascular responses to hypoxia and hypocapnia in high-altitude dwellers: Cerebrovascular responses in Andeans. The Journal of Physiology, 566(1), 287–294. https://doi.org/10.1113/jphysiol.2005.086629
Sato, K., Sadamoto, T., Hirasawa, A., Oue, A., Subudhi, A. W., Miyazawa, T., & Ogoh, S. (2012). Differential blood flow responses to CO 2 in human internal and external carotid and vertebral arteries: CO 2 reactivity in internal and external carotid and vertebral arteries. The Journal of Physiology, 590(14), 3277–3290. https://doi.org/10.1113/jphysiol.2012.230425
Scherrer, U., Vollenweider, L., Delabays, A., Savcic, M., Eichenberger, U., Kleger, G.-R., … Bärtsch, P. (1996). Inhaled nitric oxide for high-altitude pulmonary edema. New England Journal of Medicine, 334(10), 624–630.
Schneider, M., Bernasch, D., Weymann, J., Holle, R., & Bartsch, P. (2002). Acute mountain sickness: influence of susceptibility, preexposure, and ascent rate. Medicine and Science in Sports and Exercise, 34(12), 1886–1891. https://doi.org/10.1249/01.MSS.0000038894.84804.A9
Shannon, O. M., Duckworth, L., Barlow, M. J., Deighton, K., Matu, J., Williams, E. L., … O’Hara, J. P. (2017). Effects of Dietary Nitrate Supplementation on Physiological Responses, Cognitive Function, and Exercise Performance at Moderate and Very-High Simulated Altitude. Frontiers in Physiology, 8. https://doi.org/10.3389/fphys.2017.00401
Subudhi, A. W., Dimmen, A. C., & Roach, R. C. (2007). Effects of acute hypoxia on cerebral and muscle oxygenation during incremental exercise. Journal of Applied Physiology, 103(1), 177–183. https://doi.org/10.1152/japplphysiol.01460.2006
Thompson, C., Wylie, L. J., Fulford, J., Kelly, J., Black, M. I., McDonagh, S. T. J., … Jones, A. M. (2015). Dietary nitrate improves sprint performance and cognitive function during prolonged intermittent exercise. European Journal of Applied Physiology, 115(9), 1825–1834. https://doi.org/10.1007/s00421-015-3166-0
Turner, C. E., Byblow, W. D., & Gant, N. (2015). Creatine Supplementation Enhances Corticomotor Excitability and Cognitive Performance during Oxygen Deprivation. Journal of Neuroscience, 35(4), 1773–1780. https://doi.org/10.1523/JNEUROSCI.3113-14.2015
Villafuerte, F. C., & Corante, N. (2016). Chronic Mountain Sickness: Clinical Aspects, Etiology, Management, and Treatment. High Altitude Medicine & Biology, 17(2), 61–69. https://doi.org/10.1089/ham.2016.0031
Wilson, M. H., Newman, S., & Imray, C. H. (2009). The cerebral effects of ascent to high altitudes. The Lancet Neurology, 8(2), 175–191. https://doi.org/10.1016/S1474-4422(09)70014-6