
VO2max, Lactate Threshold, & VO2 Kinetics. Roller-Ski Testing with the BSF Pro Team.

At the beginning of the 2023/2024 training season, Andy Newell, head coach of the Bridger Ski Foundation Pro Team, reached out looking for help with testing some athletes in the program. With access to the Montana State University Exercise Science Lab's nordic treadmill reserved, this contract became the perfect opportunity to showcase a testing protocol I've been developing for several years. Traditional tests like VO2max or Lactate Threshold are common in endurance sports to evaluate athlete's cardiorespiratory and metabolic fitness and to set training zones (aka "levels"). However, focusing on one isolated metric such as an individual’s VO2max presents challenges in providing conclusive feedback due to its weak correlation in performance outcomes. This issue of criterion validity, meaning how accurately a test represents the outcome it was designed to measure, needs to be considered whenever we make conclusions based off of tested physiologic variables. In this case, we sought out to design a protocol that best represents performance outcomes in elite nordic skiers and provide them with accurate training levels to be used in training.
In this article, you will learn about our testing protocol, how the analysis was conducted, and the important insights found when comparing group differences.
Let’s start with the rational of why we designed the protocol the way we did. It is well known that a traditional VO2max test usually lasts only 8-12 minutes in length, because this test duration elicits the highest VO2peak values compared to longer protocols. While VO2max is an important metric, we chose a longer step-test protocol so that we could include blood lactate and VO2 kinetics all in one test. We settled for reporting ‘VO2peak,’ which was the highest 30-s average VO2 recorded during the final stages of the test. With this in mind, the ‘VO2peak’ values do not represent the true ‘VO2max’ of each athlete. I would estimate that if we followed a traditional VO2max running protocol, we would see VO2peak values 10% higher than what is reported.
When taking blood lactate measures, the intensity “steps” need to be long enough to observe lactate values stabilize. These steps can vary anywhere from 3-10 minutes. Less than 3-minutes and you will see irregular lactate values. Too long of steps and you will subject the athlete to muscular fatigue and depletion of glycogen, inhibiting how deep into the protocol they can go. We chose 4-mins as this is relatively standard within other testing protocols.
Between steps, we included a 1-minute recovery phase. We included a recovery phase to 1.) safely procure a blood lactate value on the treadmill and 2.) provide the opportunity to analyze the VO2kinetics of transitioning between rest and the subsequent testing stage.
Therefore, our testing protocol was designed to measure/identify the following variables:
Lactate Threshold Profile
VO2 uptake kinetics
VO2 peak
VO2 at thresholds
Heart Rate Training Levels
Caloric Expenditure
Measures of ventilatory function
Analysis of intensity domains (Moderate, heavy, & severe domains)
Protocol
15-minute warm-up on Nordic treadmill
4-min stage incremental step-test until blood lactate rose above 6 mmol/L. This test was designed to reach near-maximal conditions in 6-10 stages; however, we did not push participants to task-failure or volitional fatigue.
There was 1-minute of rest between 4-minute stages. During this recovery interval, athletes stepped off treadmill and we measured blood lactate and allowed VO2 to recover.
Threshold determination techniques:
The standard view-point of a majority of exercise physiologists, is that there are 4-exercise intensity domains (moderate, heavy, severe, & extreme) that help define how one’s physiology is functioning in relation to exercise intensity. There are numerous techniques to identify the thresholds that separate these exercise intensity domains. Below, I’ve described the techniques I considered when identifying these transition points.
When identifying the transition between the moderate and heavy exercise intensity domains, we considered the following parameters:
An increase in lactate above baseline values (lowest recorded) >.3 mmol/L.
The first presence of a slow component rise in VO2 kinetics following the primary phase, signifying the heavy domain.
A deviation in the slope of a VE/VO2 trend line (see Figure 1), where an increase in VE is detected relative to VO2, which leads to a nadir and/or "flattening" of the trend line before the trend line begins to rise in relation to increasing exercise intensity.
This transition point is often referred to as the 1st lactate threshold (LT1), 1st ventilatory threshold (VT1), or the aerobic threshold (AeT).
* VE= minute ventilation (L/min)
* VO2 = volume of oyxgen consumption (mL/kg/min)
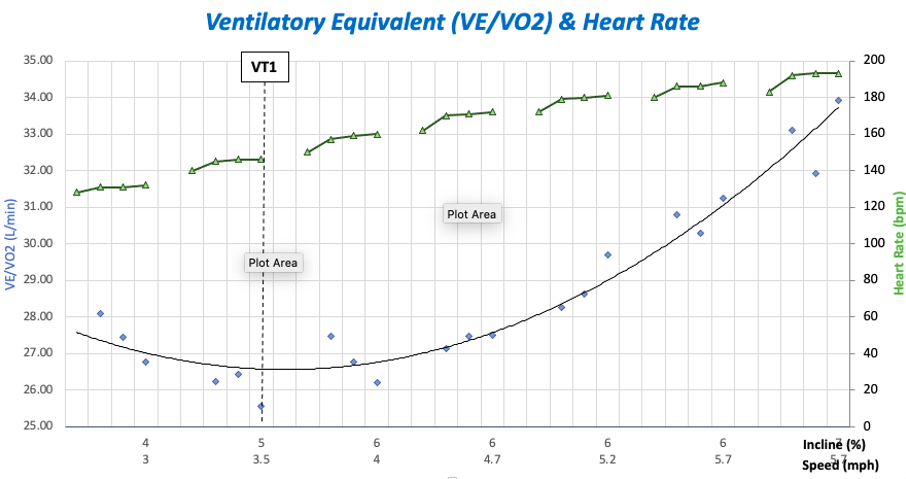
Figure 1 Relationship between Minute Ventilation (VE) and Volume of Oxygen Consumption (VO2) to determine the boundary between the moderate and heavy exercise intensity domains
When identifying the transition between heavy and severe exercise intensity domains, we considered the following parameters:
Dmax-modified method. This is identified as the point in the lactate profile polynomial trendline where lactate begins to rise exponentially (see Figure 2). The furthest distance between the trendline and the D-max line (drawn from LT1 to the maximal lactate value), signifies the 2nd Lactate Threshold (LT2). LT2 represents the point where lactate disposal has reached its maximum rate, and lactate therefore rises exponentially.
Lactate at 4 mmol/L. *Note this does not apply to all.
A sudden increase in the ratio between tidal volume and ventilation (VE/Tv). This represents the point where athletes begin to breathe more frequently due to the accumulation of metabolic acidosis and therefore CO2 in the blood.
This transition point is often referred to as the 2nd lactate threshold (LT2), lactate turn point (LTP) 2nd ventilatory threshold (VT2), or the anaerobic threshold (AnT).

Figure 2 Lactate Threshold profile used to determine exercise intensity domains
Setting Heart Rate Training Levels
The thresholds of LT1 and LT2, which determine the intensity domains, were used to identify the boundaries of heart rate training ranges, also known as levels. The transition between the moderate and heavy domains represents the transition between Level 1 & Level 2 heart rates. Whereas the transition between the heavy and severe domains represents the transition between Level 3 & Level 4 heart rates. A lower Level 1 range, calculated as 90% below LT1, was also identified, as this training zone is recommended for certain workouts. This was calculated as below 90% of LT1 heart rate. See Figure 3 for calculation methods.

Figure 3 Example of heart rate training levels based on LT1 & LT2 determination

VO2 Kinetics Analysis
VO2 Kinetics refers to the "responsiveness" of your aerobic system when there is a rapid change in exercise intensity. In other words, the time that is required for oxygen consumption to increase its contribution to the match energy demands of a given workload. This physiologic parameter is measured as "tau," which is a time constant value that tells us the length of time it takes for VO2 to increase 63% of the total amount required of a given task. While this metric may sound complicated at first, its application is much easier to comprehend in practice (see Article: Physiology Explained: Energy Systems & VO2 kinetics of MTB training for more information)
Figure 4: VO2 kinetics of a well-trained skier exercising in the heavy domain
For instance, once you have measured tau for a given intensity, simply multiple the time constant by 4 to predict how many seconds it would take for the aerobic system to meet the energy requirement for a given task. Furthermore, if the intensity is below LT2, then we can assume they have reached steady-state conditions.
In the example from Figure 4, the measured time constant was 27 s, meaning at this intensity it will take 108 s (4 x 27s) to reach full steady state VO2. In this example, the athlete was exercising in the heavy domain (>LT1) at a blood lactate accumulation of 2.1 mmol/L.
Having fast VO2 kinetics is important for endurance athletes due to the implications of what occurs leading up to steady state metabolism, where the aerobic system is matching the energy demands of a given intensity. This timespan, known as the oxygen deficit, is where the phosphocreatine and glycolytic systems are producing energy anaerobically until the aerobic system catches upto match energy demands. While these anaerobic systems produce energy more rapidly than the aerobic system, the downside is the accumulation of harmful waste products such as hydrogen ions (H+) and inorganic phosphates (Pi), which cause metabolic acidosis and impair muscle contraction. Furthermore, the reserve of glycogen and creatine phosphate equates to a fraction of the energy obtained from free fatty acids.
This reserve can also be depleted during longer endurance events performed in the heavy domain, especially when there are intermittent changes in exercise intensity causing an accumulation of oxygen deficits. An example would be running on a flat marathon course at a constant pace versus a course with intermittent hills and stochastic pacing strategies.
From recent research on elite endurance athletes in the Breaking-2-hour marathon project, Jones et al (2021) found that the time constant, tau, was the only physiologic variable significantly correlated with marathon performance. This means that VO2 kinetics predicted marathon performance better than VO2peak, running economy, and any lactate related metric in isolation. It was only when those latter variables were considered together did they see significant correlations with best marathon performances. For example, with a VO2max of 80 ml/kg/min, a lactate threshold of at least 85% of VO2max, and a running economy of 190 mL/kg/km someone could predictably maintain the marathon pace required of 4:30 min/mile to break the 2-hour barrier.
Given this research, we decided to try and include the primary phase time constant, tau, as one of performance metrics in this group. Using an open-source code for VO2 Kinetics analysis software called VO2 Fitting, we were able to complete VO2 Kinetics analysis on all stages of the test for each participant.
Link to URL software access: https://mgreene.shinyapps.io/kinetic-vo2/
As this was not a traditional VO2 kinetics protocol, there were some limitations to consider:
1. VO2 kinetics can be affected by prior exercise. This phenomenon is known as "priming" where we can see an increase in the speed of VO2 kinetics from previous exposure to exercise in the heavy and severe domains.
2. The stage-length of only 4-minutes is shorter than traditional VO2 kinetics tests where we may aim for 6-minutes. However, this limitation may only affect the analysis of the slow-component time constant.
Lactate Profile Physiology
Undoubtedly, a lactate threshold profile is one of the best ways to assess endurance capacity. When analyzing a lactate profile curve, there are several key factors that represent physiologic determinants of performance for endurance athletes. Generally for endurance athletes, we should aim to strive for a Lactate Profile that is low as possible in the moderate and heavy domains. This is especially true the longer the event is. In the moderate domain, I look for the lowest values on the curve. For instance some well-trained individuals can exercise at a lactate < 1 mmol/L whereas some untrained individuals lowest lactate value may be > 3 mmol/L. In the heavy domain, I look to see if lactate begins to rise quickly towards LT2 or if rises slowly. The latter implies a well-developed aerobic base and the ability to sustain intensities in the heavy domain for long periods of time. For most athletes, we want to see LT2 occur at the highest percent of VO2peak possible. In other words, the fastest speed, power, incline, etc. before lactate disposal has reached its physiologic max. Lastly, during protocols designed to reach VO2max, or volitional fatigue, the final lactate measurement (Lamax) is of interest as it implies the “glycolytic capacity” or an individual. I see a wide range in this anywhere from 4 - 14 mmol/L. When testing ultra-marathoners, I will commonly see a Lamax of only 4-6 mmol/L. Whereas endurance athletes who engage in short-bursts of high intensity such as mountain biking, I see a Lamax usually between 9-14 mmol/L.
Each blood lactate measurement completed at the end of a 4-min stage represents the balance between lactate production and clearance at a given intensity. Lactate production, known as the rate of appearance (Ra), is dependent on several factors including:
(1) The rate at which energy (ATP) is needed for a given exercise intensity (i.e. sprinting vs. slow jogging).
(2) The contribution of glycolysis, which is the breakdown of glucose or glycogen (glycogenolysis), to meet the energy requirements
(3) Recruitment of fast twitch fibers, which are known to have higher glycolytic capacities and therefore produce more lactate
(4) MCT4 Lactate transporters, which shuttle lactate out of a muscle cell and into the blood stream. MCT4 transporters are more active in high-intensity focused athletes (i.e., higher in 800 m runners than marathon runners).

Figure 5: Comparison of Lactate Profiles between Athlete 1, 2, & 3.
In contrast, lactate clearance, known as rate of disposal (Rd), is dependent on the following factors:
(1) Slow twitch muscle fiber distribution. Slow twitch fibers have high mitochondrial density and consume lactate as a substrate for aerobic metabolism.
(2) Fat burning capacity. Lactate and fat metabolism can be viewed as being inverse of one another. When lactate levels are lowest during a test (LTmin), fat burning is likely at its highest rate (and vice versa). So the greater contribution of fat as fuel, the less one needs to rely on glycolysis.
(3) MCT1 Lactate Transporter, which shuttle lactate from the bloodstream into oxidative muscle cells to be oxidized. MCT1s are highly expressed in slow twitch skeletal muscle fibers and cardiac muscle fibers.
Group Differences
We found significant differences in several physiological variables throughout the group which are outlined in Table 1 below. Using a few examples, I’ll explain what the implications are of some of these variables. The main comparisons will be between athletes 2 & 3 and athletes 4 & 5. Athlete 1 is a sprint-focused skier who had a lower relative VO2peak of 56 mL/kg/min, VO2 kinetics averaged at 27.5 s, and a lactate profile that shows an earlier onset of lactate accumulation. This led to an earlier termination of the test at the 5.8 mph stage. From this information, we can infer that this athlete is fast-twitch muscle fiber dominant and does not recycle lactate as efficiently as athlete 2 & 3. This athlete’s main events consist of sprints usually lasting 4-mins or less so these physiologic factors matter less compared to athletes who’s competitions last longer durations. More appropriate tests may include critical speed testing and Wingate testing to understand his anaerobic capacities.

Table 1 Group differences in average Tau of primary phase, minimum Tau P measured, absolute VO2peak (mL/min), relative VO2peak (mL/kg/min), VO2 at LT1, VO2 at LT2, and lowest lactate value - LTmin (mmol/L).
In figure 6, we can compare the difference in the primary phase kinetics between two athletes in the testing group. During this testing stage, the athlete’s roller skied for 4-mins at 6% incline and 4 mph. For each athlete, this was the 3rd stage of the test and there was 1-min of full rest before starting this intensity. In figure 5A, the primary phase time constant, tau, was measured at 18 s, whereas in figure 5B, tau was measured at 39 s. Interestingly, athlete 4 had a lower blood lactate concentration during this stage at 1.8 mmol/L, whereas athlete 5 had a higher blood lactate concentration at 2.1 mmol/L. In figure 5B, you may also notice the presence of a slow component rise after the initial primary phase, indicating a higher VO2 cost to complete the same exercise intensity. These differences indicate that athlete 4 can be classified as exercising in the moderate domain whereas athlete 5 was exercising in the heavy domain. For more information on primary and slow component VO2 kinetics, refer to previous blog: “Physiology Explained: Energy Systems & VO2 kinetics of MTB training.”

Figure 6 VO2 kinetics comparison between athlete 4 (A) and athlete 5 (B) during the 6% incline / 4 mph stage.
Given this information, we would want to start implementing some strategies that improve athlete 5’s VO2 uptake kinetics. This metric implies a greater reliance on the anaerobic energy systems and recruitment of fast twitch muscle fiber at a lower intensity compared to athlete 4. Generally, increasing annual training hours at intensities < LT1 can improve this metric. Exercising more in the moderate domain ensures a greater stimulus on slow twitch muscle fiber without inducing too much autonomic stress. However, this process should be carefully planned out to fit the annual training cycle and to avoid ramping up volume too quickly. For instance, if this athlete increased annual training hours from 500 hrs/year to 700 hrs/year, this may impede with other important training qualities. Simply, if more hours are added and the athlete can not tolerate the stress, a more conservative approach should be taken.
When comparing the primary physiologic variables of VO2peak, VO2 kinetics, & Lactate Profiles between Athlete 2 & 3, we found several differences that suggest 1) each athlete may be better suited for events more suited to their physiology. 2) there may be some changes to training variables such as training volume and intensity distribution that could improve physiologic limiters to certain events and 3) there is no “perfect physiology, ” rather there are multiple components that make up an athlete and there are many ways to develop an athlete towards peak performance.
Athlete 3 had a higher VO2peak of 5870 mL/min compared to Athlete 2 with a VO2peak of 4980 mL/min. Athlete 3 does have higher body mass of 84 kg compared to Athlete 2 at 75.5 kg. With the weight-adjusted relative VO2 peak, Athlete 3 still had a higher relative VO2peak of 69 mL/kg/min compared to Athlete 2 who had a VO2peak of 66 mL/kg/min.
When comparing Lactate profiles (figure 5), you can see that Athlete 2 demonstrates a slower onset of blood lactate accumulation and reaches LT1 and LT2 at higher speeds on the treadmill. Greater lactate clearance capacities in combination with faster VO2 uptake kinetics, expressed as tau, suggests that Athlete 2 is more of a slow-twitch dominant athlete and may excel more in longer distance events whereas athlete 3 may excel more in middle distance events. Athlete 2’s tau constant of 11-s in the moderate domain is actually similar to what was observed in the elite marathoners studied in the breaking 2 project. Whereas athlete 3’s tau constant of 20-s indicates a slightly greater contribution from anaerobic energy systems at the onset of exercise.
Making recommendations to elite athletes to improve such specific parameters needs to come with the understanding that all events require different physiologic capacities. An athlete can either make changes to training structure based on testing results (e.g. more volume, more intensity, etc.) to better prepare for an event or they can try to understand the type of events that best suit their physiology. Ultimately, these decisions should only be addressed once the basics are executed and an athlete is ready to achieve their highest potential.
Acknowledgments:
I would like to thank Dr. Erin Smith for help editing and reviewing this paper, Mac Greene for setting up the VO2 kinetics analysis software, and Dr. Dan Heil for letting us use his lab space at MSU.
References:
Physiological demands of running at 2-hour marathon race pace
Andrew M. Jones, Brett S. Kirby, Ida E. Clark, Hannah M. Rice, Elizabeth Fulkerson, Lee J. Wylie, Daryl P. Wilkerson, Anni Vanhatalo, and Brad W. Wilkins
Journal of Applied Physiology 2021130:2,369-379